
Patellar latendinopathy is a common cause of pain in the anterior knee, which is characterized by pain that is localized at the lower pole of the patella under load.
There are a number of risk factors for the development of patellar tendinitis, but an exact and specific cause is unknown. Until recently, the condition was known as patellar tendinitis, which suggests an acute inflammatory cause. However, from histological studies we know that this is not true, as the main feature of the disease is degenerative changes in the tendon rather than the presence of inflammatory cells . Therefore, the disease was renamed Tondinopathy to reflect the degenerative and chronic cause of the disease.
Since there is only minimal acute inflammatory involvement in the disease, anti-inflammatory medication is not effective, since there is no acute inflammatory process to be disturbed.
The most widespread treatment of patellar endinopathy is eccentric exercise therapy (EET) after a short rest period. Programs like Malliaris et al. (2015) are widely used in clinical practice and recommended by NICE. However, these exercises can be painful and irritable. There is also some debate about its effectiveness in allowing early return to work.
Eccentric load plan by Malliaris et al. (2015)
For several years there has been increasing evidence of an alternative and less pain-inducing treatment than eccentric stress; progressive tendon loading exercises within pain limits (PTLE). Although the move from EET to PTLE is increasingly supported anecdotally and logically, there is limited evidence comparing the effectiveness of the two approaches. The new JUMPER study aimed to compare PTLE and EET based on the clinical result after 24 weeks in patients with patellar endinopathy.
Dive deep into cones with Ebonie Rio
Methods
The JUMPER study was a stratified, single-blinded RCT in which athletes of all ability levels participated. Inclusion criteria:
Age 18-35
History of knee pain in the patella caused by exercise / competition
Take part in sport at least 3 times a week
Structural tendon changes in USS / Doppler
VISA-P score of <80/100
Participants were excluded if: an injury was acute, previous knee surgery without full rehab, known inflammatory disease, daily use of medication or a recent injection that affects the tendon, high cholesterol, previous tendon ruptures, and Impairment of performance in the exercise program, participation in another study / treatment program, or signs of another knee pathology. Details on clinical investigation and randomization can be found in the article, which is free and openly accessible and referenced at the end of the text.
The primary result was a VISA-P questionnaire which was completed at the start of the study after 12 and 24 weeks. Secondary outcomes were return to exercise, exercise compliance, and patient satisfaction. A total of 76 participants were randomized into the trail, 67 made it to the end of the 24 weeks.
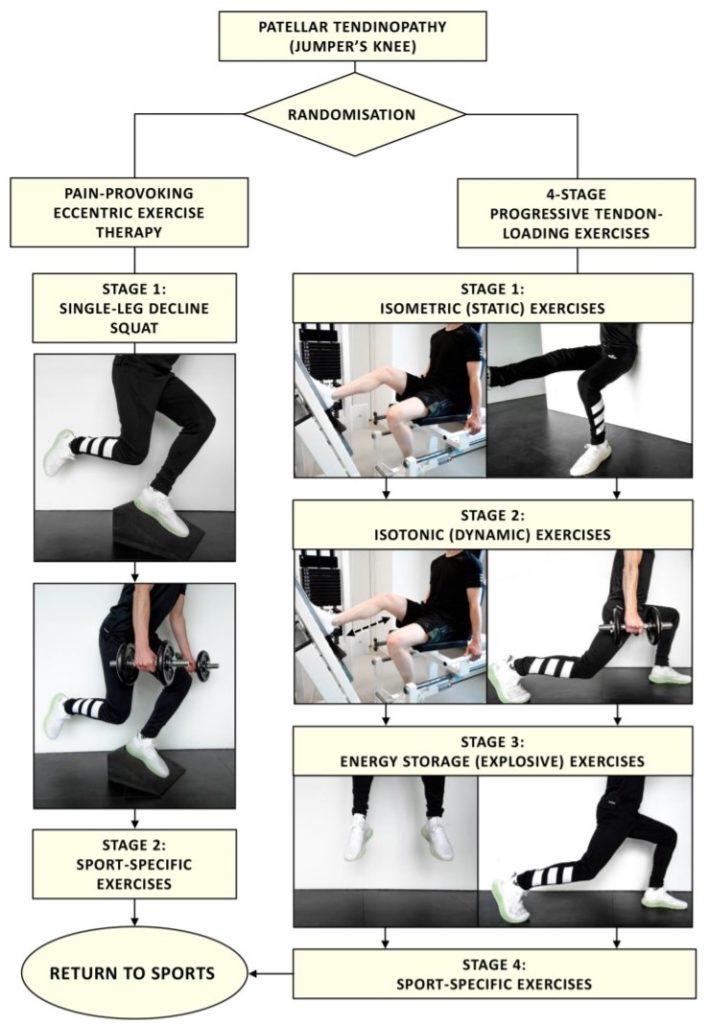
Intervention
The patients were randomly assigned to PTLE for 24 weeks within the limits of acceptable pain (intervention) or pain-inducing EET (control). Training plans and videos were available to all patients via the study website (currently inactive) and via training brochures (currently not accessible).
Patients in the intervention group performed static isotonic, explosive and sport-specific exercises within the pain limits, one after the other. The progressive load was adjusted according to the individual reaction (use VAS).
The PTLE program consisted of 4 phases:
Level 1: Daily isometric exercises (single leg press / leg extension) Isometric 5×45 medium range quads at 70% MVC.
Level 2: Level 1 exercises on the first day and new isotonic exercises on the second day. These exercises were also performed as a one-legged leg press or
leg extension and began with 4 × 15 repetitions between
10 ° and 60 ° knee flexion and slowly progressed to 4 × 6
. Repetitions with increasing load and knee angles between almost
full extension and 90 ° flexion.
Level 3: plyometric loading and running exercises (jump squats, box
jumps and cutting maneuvers) on every third day, starting with
3 sets of 10 repetitions with both legs and slowly progressing
for 6 sets of 10 repetitions with one leg. Isometric and isotonic
exercises were continued on every first and second day, respectively.
Level 4: sport-specific exercises that were characteristic of the sport. Patients were instructed to gradually return to exercise-specific training, which was performed every 2 to 3 days, to recover from exercises with high tendon stress. In this phase, the isometric exercises of phase 1 were continued on days when the sport-specific exercises were not performed.
Progression to each subsequent stage was defined using individualized progress criteria based on the level of pain experienced during a pain provocation test consisting of a single leg squat. If the VAS score was 3 or less and the level exercises were performed for at least 1 week, it was recommended to move to the next level. If all Level 4 exercises were performed within acceptable pain limits (VAS score ≤3 points), then return to competition was recommended.
After returning to sport levels 1 and 2, maintenance exercises were recommended twice a week. The fastest possible time to get back to exercise after this PTLE program was after 4 weeks.
Dive deep into cones with Ebonie Rio
The EET control group performed their exercises twice a day for 12 weeks. The exercises were carried out on a lowering board with an incline of 25 degrees. Stage 1 of the EET consisted of a one-legged squat, in which the downward component (eccentric phase) was performed with the symptomatic leg and the upward component (concentric phase) was performed primarily using the contralateral leg. Patients were instructed to perform the exercises with pain (VAS score ≥ 5 points on a scale of 0 to 10 during the exercises).
Level 2 was initiated when the level 1 exercises were fully complied with and when acceptable pain occurred during eccentric exercises with additional weights (VAS score ≤3 points on a scale from 0 to 10; the number of weights was not specified ).
Level 2 exercises consisted of sport-specific exercises that were characteristic of the type of sport. The maintenance drills consisted of level 1 drills twice a week. Patients in the EET group were allowed to exercise again after 4 weeks. We recommend doing this when a one-leg squat can be performed within acceptable pain limits (VAS score ≤3 points on a 0-10 scale). The acceptance plate with an incline of 25 ° was provided for patients who were assigned to the EET
Clinical implications and results
In this RCT with 67 patients, progressive tendon loading exercises were more effective than eccentric loading exercises with regard to patient satisfaction, VISA-P score and return to sport within 24 weeks.
Brief summary of the results
VISA-P improved from 56 to 84 in the treatment group and 57 to 75 in the control group.
The difference between the PTLE and EET groups was not significant after 12 weeks, but was significant after 24 weeks in favor of PTLE .
In the PTLE group, 21% returned to pre-injury exercise after 12 weeks and 43% after 24 weeks.
There is no difference in compliance with exercises but the PTLE group was far more satisfied with their program than the EET group
It is important that we do not outdo ourselves and radically change our clinical practice at this stage, as this is an RCT of 67 people. For some patients, PTLE may be a more suitable option than EET, especially if they do not stick to eccentric exercises or if they find it too irritable and therefore not advisable to stick to the program.
It has to be taken into account that the participants had or mixed sporting skills and performances, and therefore it is not possible to draw firm conclusions about whether or not this affects the effectiveness of PTLE or EET. The results could be more specific for both population groups if the study were designed differently.
In addition, the exercise was unsupervised and was performed on a patient population who are familiar with technical exercises. The results in a population that is not familiar with this level of technical training are likely to be different. To counteract this supervised exercise, it may be necessary at least for the initial phases of the exercise program.
Another restriction is that if the worst-case scenario of the sensitivity analysis of missing data is correct, the better clinical result of the PTLE group no longer applies. However, this worst-case scenario is unlikely.


